Featured Article:The Islamic State Healthcare Paradox: A Caliphate in Crisis
By
2015, Vol. 7 No. 07 | pg. 1/3 | »
IN THIS ARTICLE
KEYWORDS
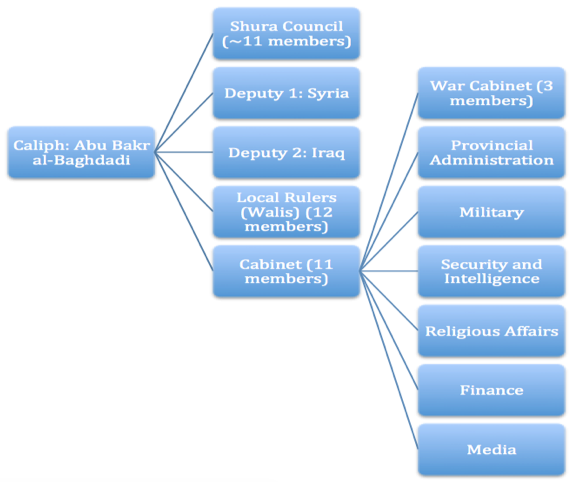
AbstractThe civil war in Syria has taken an enormous toll on civilian populations. One of the most commonly overlooked aspect of this crisis is the impact on healthcare in the region. Syria’s health capacity has been ravaged by years of government bombings and Islamic State expansion. As the Islamic State (IS) continues to consolidate territory, its actions become less and less clear. Islamic State militants have embarked on a brutal campaign against health providers and infrastructure, yet they attempt to promote health among other social services in order to gain support from local populations in controlled territories. What, then, is the Islamic State's strategy on health? How does it create a functioning apparatus for social service delivery, and more specifically, for healthcare delivery? How can the international community exploit this knowledge in order to internally cripple the Islamic State by turning its own health architecture and philosophy against itself? In this paper, I explore these questions and provide an analysis of relevant news coverage, academic literature, and eyewitness accounts in Syria and Iraq in order to make the case that healthcare provides a crucial avenue of understanding and, ultimately undermining and destroying, the Islamic State. Health as an Instrument of Warfare“One doctor in Mosul said that earlier this month, he witnessed a patient arguing with a physician affiliated with the Islamic State. The next day, militants brought the patient to the hospital lobby, where they whipped him and forced him to apologize to the physician. “Of course, those of us who didn’t join them, we are all living in fear” - Personal Account from a Syrian Physician (Cunningham) In Arabic, there is an adage that claims “المؤمن مصاب (il-mo'men muSaab),” which in English roughly translates as, “The righteous always suffer.” Since the onset of the Syrian Civil War in 2011, following what was at the time a peaceful protest by righteous civilians against a savage, authoritarian regime, a variety of social structures have collapsed, corroding the essential fabric that holds Syrian and Iraqi civil society together.Social dynamics, having been exploited by all actors in the conflict, have internally disintegrated, exposing brutal sentiments among government bureaucrats, civilians, and insurgents engaged in oppressive Jihad. The scale of the conflict has expanded over three years of instability, and the tides have turned in favor of The Islamic State of Iraq and the Levant (ISIL), alternatively referred to as “The Islamic State (IS)” or “Daesh” in Arabic. The war thus far has been viewed primarily from a military perspective, concentrating on varied prescriptions of armed force to combat the growing extremist threat. Against the backdrop of military and politics within this conflict bubble, however, has existed a largely ignored yet crucial narrative of civilian life, most notably in the health sector. One of the most distressing aspects of the war has been the sheer devastation of health architecture throughout Syria and IS-controlled regions in Iraq, alongside the persistent denial of aid delivery, access to care, and health infrastructure as a means of protecting wounded and fleeing civilians (Johns Hopkins University). The injuries to both civilians and institutions have been catastrophic, and in many ways, reflective of a helpless people trapped in a tug of war between government and terrorist oppressors. In the past three years of the war, Syrian armed forces and Islamic State extremists systematically targeted civilians followed by their health facilities and personnel, reflecting a new and horrific trend—a trend which highlights a departure from previous wars—in which the norm is no longer the indiscriminate devastation of health infrastructure, but rather one of the primary goals of the oppressing faction. Since its rise in 2014, the Islamic State has stormed and bombed hospitals treating wounded civilians, abducted and assassinated patients and health providers, and imposed restrictive measures against women, serving a dehumanizing function that has led to the mass exodus of medical personnel out of Syria (Gutman). Kurdish media reports indicate that IS militants have been targeting and killing physicians that refuse to provide treatment for wounded IS soldiers (Porter, Halevy et. al). Last December, for example, an element of IS executed two top emergency surgeons within the Mosul Health Department by firing squad for their unwillingness to transfer to a field hospital (Rudaw). This mass campaign against physicians has been wholly arbitrary, unnecessary, and merciless. The situation for women has been particularly concerning from a standpoint of human rights. Female doctors interviewed about conditions in IS-controlled hospitals explain that in Mosul, women are denigrated as objects of a religious will, and rather than being viewed as providers of service, women are objectified as receivers of the terrorists’ imposition of control. Female practitioners who do not wear a veil over their face at health facilities are barred from entering hospitals (Abhoud). A Syrian female gynecologist reflects on a time when she was scheduled to perform a surgery, but because she was not wearing a veil, she was denied access to the surgical ward. The IS militants told her to “let the patients die…what matters is your veil (Abhoud).” Accordingly, in the IS stronghold of Raqqa, hospitals are almost completed devoid of female doctors, and the few nurses that exist are forbidden to work in a healthcare setting without permission and physical company of a male mahram, a designated male watch guard (Mahmood). What’s more, IS militants have subjugated and sexually abused women and girls in controlled areas as documented by UN reports (Fick). Clearly, from a human rights angle, the atrocities perpetuated and magnified by IS factions have created an exceptionally hostile environment for healthcare providers, fundamentally altering the dynamic of the war against civilians who are constantly barraged by government weaponry and militant barbarity. In many ways, there seems to be little hope for survival, ergo the only solution is to flee, intensifying many pre-existing spillover issues, such as refugee displacement, unstable medical geography, and mass death. The consequences are very plainly expressed via statistics compiled by the Syrian American Medical Society and the WHO: approximately 60 percent of hospitals have been destroyed, 90 percent of the local pharmaceutical industry has been destroyed, 78 percent of ambulances are severely damaged, and 70 percent of whatever medical staff is left cannot access their workplaces (Al-Jadda). In certain provinces, upwards of about 90 percent of all physicians have left or have been killed, and in the stronghold of Aleppo, less than 250 physicians are left, creating a physician-to-patient ratio of about 1:500,000 (Johns Hopkins University, Al-Jadda). Polio has returned to Syria after fourteen years, and infectious disease outbreaks are on the rise as the provision of vaccinations has fallen drastically (Al-Jadda). Granted, The Islamic State is not the sole culprit for the majority of these issues; Physicians for Human Rights found that the Syrian government is overwhelmingly responsible for the deaths of medical personnel throughout the country (PHR). Nevertheless, though it is important to attribute culpable actors wherever necessary, I will focus on the Islamic State because its intentions are far less clear than those of the Syrian government; the Syrian government’s intention is to destroy all medical facilities capable of supporting rebel forces. Thereby, the easiest mechanism through which the government can destroy the rebel population is by targeting the health facilities. The potential short-term solutions to mass health catastrophe for most wars would be the obvious provision of healthcare by international agencies and relief organizations. This is not the case with The Islamic State. Not only has IS refused to negotiate with international third parties to allow for foreign medical aid delivery (Reuters); in Al-Hasakah governorate, for example, IS obstructed the importation of medicine for hundreds of thousands of people (Cunningham). The Two Faces of Daesh: The Islamic State Healthcare ParadoxThe Islamic State is an anomaly among all terrorist organizations that have operated following the commencement of the War on Terror. Wherever IS gains territory, they seek to consolidate control in a central governing body and declare the rule of law over the local population. Hence, the organization embarks on a campaign that is in some ways ironically diametric to many actions they simultaneously commit. For example, while executing doctors, bombing hospitals, and sexually oppressing females, IS militants demonstrate to local people that they are capable of running a city and thereby provide social services for the locals (Wellen). Compounding these seemingly disparate actions lies the paradox in the notion that IS is attempting to build its own healthcare system. In April 2015, the Islamic State released a new propaganda video boasting a new healthcare system with advanced medical schools and emergency care equipment to treat citizens in controlled areas. Analogous to the North Korean’s state-sponsored totalitarian propaganda scheme, IS marketing and promotional strategy radically exaggerates its healthcare capacity in an attempt to grow its “service” and recruit foreign physicians to operate in IS-controlled areas (Bacchi and Limam). The service, modeled after the British National Health Service, features a savvy commercial with high-end technologies that rival those of advanced hospitals in Western countries. The strategy has been working effectively. A number of British medical students and doctors recently traveled to Syria to work in controlled areas (Bennhold). Once they are there, however, the reality of the situation strikes. Citizens in Raqqa report that even in the areas with the most optimal healthcare facilities and capacity, militants are given priority in special areas restricted for their families (I24 News). Often, civilians are left outside the system. These features of the war create enormous confusions. On one hand, IS systematically targets and eradicates any healthcare infrastructure that could otherwise serve its own interests; on another hand, IS recruits doctors, promotes health as a service for all, and provides social services to earn the respect of the local people. One face of IS is callous and calculative; the other face is compassionate and solicitous. Why? Another tier of confusion layers itself on these questions. Local Middle Eastern news outlets report that militants from IS have been infected by a skin disease called “Leishmaniasis” that creates large open wounds that eat away at human flesh. The disease is spread by poor hygiene conditions and pollution, and Raqqa—once again, an IS stronghold—is facing the highest risks of contracting the disease (Al Arabiya News). Doctors representing international relief agencies like Medicin Sans Frontiere have tried to cure the disease but are prevented from accessing IS-controlled regions (Al Arabiya News). Since medical centers have closed or been destroyed, the disease has become acuter (Siegel-Itzkovich). As a result, local medics or physicians left in deplete areas have little experience dealing with the disease, and the disease accordingly spreads rapidly. In Aleppo, more than 100,000 cases of Leishmaniasis have been reported, and a breakdown in access to pharmaceuticals has begun to internally cripple civilian populations and IS militants themselves (Cooper). Given the fact that a militant-crippling disease is on the rise, the people whom IS purportedly protects are increasingly marginalized from healthcare opportunities, and the capacity to diagnose and treat medical problems is decaying, IS must reorient its philosophy towards health and its actions on the ground if is it to endure these conditions effectively. Dissecting Bureaucracy: The Islamic State Governance Model and Medical ApparatusHow has the Islamic State adapted itself to the challenges of governance and disease growth? How does IS administer significant financial resources on social service delivery? Documents obtained by German media outlets shed light on these complicated matters; a close look at IS’s structure reveals a highly organized bureaucratic system operating on many similar levels as would a state (Deutsche Welle). After capturing municipalities through brute force, suicide bombings, and calamitous violence, IS attempt to ensure an “egalitarian provision” of services, most applicable to infrastructural needs like electricity, water, gas, and food (Lister). To expand its ravaged healthcare capacity, IS opened a “free” hospital (note that free largely pertains to fighters as outlined above) in Mosul after its capture (Lister). In many ways, The Islamic State has the fundamentals for a working state apparatus: IS manages its people through police and security forces, operates a health system (albeit very poorly), provides social services for individuals, and operates a justice system based on sharia law. IS employs between 20,000 – 31,500 fighters alongside administrative staff who serve from abroad or who stay in their positions (Barrett). To persuade workers in existing state apparatuses to retain their positions following IS-takeover, militants provide said workers with a consistent salary. However, to prevent disloyalty, essential staffs—Islamic State supervisors—oversee operations in all facilities and departments. The Islamic State hierarchy is as follows: A single self-proclaimed caliph, or religious leader, in this case, Abu Bakr al-Baghdadi, is the first-in-command, and unlike many bureaucracies, he both has ultimate authority in any matter and often interferes with a majority of high-level decisions which are executed by other lower-tier councils or people. The entire vision of the terrorist network is implemented under his oversight at all times, and much like a totalitarian leader, he has his hand in most state matters. Abu Bakr has two deputies who respectively oversee operations in Syria and Iraq and with whom Abu Bakr sets overall strategic objectives of the Islamic State as a whole (Barrett). Below Abu Bakr, the caliph, and his two deputies enlist 12 local rulers called walis, a Cabinet comprised of eleven officials, three of whom operate a War Cabinet, and eight others who respectively oversee Councils on Provincial Administration (civilian matters like health), Military, Security/Intelligence, Religious Affairs, Finance, and Media (Barrett). An additional Shura Council separate from the central cabinet advises Abu Bakr on sharia principles of the organization; the Shura Council, much like Western democratic structures, is a body of approximately 11 members that has the power to dismiss the Caliph should he fail his duties (Arango et. al).
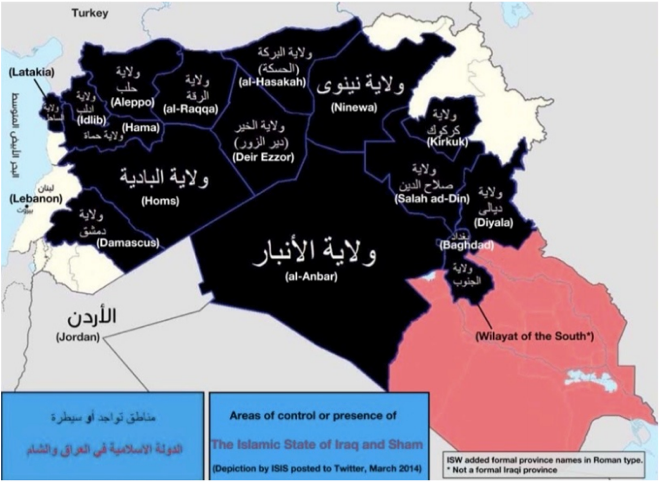
Figure 1. Map produced by the Islamic State to show its presence and administrative divisions in March 2014, before the creation of Furat and Fallujah provinces. From Barrett (2014). Rationalizing the overall structure gives one a better understanding of how, much like a state, the Islamic State operates to provide healthcare for its citizens. The Provincial Council is our council of interest, as it is divided into 18 provinces, with a governor for each province who presides over the local structure for civilian administration (Arango et. al). Each governor is responsible for coordinating funding of infrastructure and capacity building projects along with running programs like healthcare (Friedland). Out of all the cities under IS control, Raqqa, which has established itself as a de facto capital of The Islamic State, is the most developed governorate with the widest range of social service delivery. The governorates, as drawn by The Islamic State itself, are shown in Figure 1. Below is a simplified diagram summarizing my research on the power divisions within the Islamic State governing apparatus (Figure 2):
The Provincial Administration is divided into their respective departments like education, healthcare, etc., but the enforcement of those departmental specifics lies within the jurisdiction of the governors for each region. The Health Department—The Diwan al-Siha—presents itself as a guarantor of health services along with establishing regulations for smoking, consumption of alcohol, recruitment of volunteers and medical personnel, pharmaceutical price controls, gender segregation, medical supply distribution, etc. (Al-Tamimi). The subdivisions of each governorate’s authority complicates the bureaucracy further, and for the purposes of time and relevancy, I refrain from more specifically describing those agencies. A marked distinction with The Islamic State is its use of local bureaucrats already in charge of hospitals, law enforcement, and municipal services to remain in their positions as to avoid inadvertent placement of a fighter in a position of administrative authority—a situation that could prove deleterious to the welfare of both fighters and civilians (Dreazen).Continued on Next Page » 
From the Inquiries Journal Blog  ") Related ReadingMonthly Newsletter SignupThe newsletter highlights recent selections from the journal and useful tips from our blog. Suggested Reading from Inquiries Journal
Inquiries Journal provides undergraduate and graduate students around the world a platform for the wide dissemination of academic work over a range of core disciplines. Representing the work of students from hundreds of institutions around the globe, Inquiries Journal's large database of academic articles is completely free. Learn more | Blog | Submit Follow IJ
Latest in Political Science |