In the American healthcare system there have been few trends as persistent, yet avoidable, as the rise in prescription drug overdoses. Between 1999 and 2008 prescription overdoses quadrupled to nearly twenty thousand per year (Paulozzi, Jones, Mack, & Rudd, 2011). It is estimated that nearly six million Americans are abusing or misusing prescription drugs in any given year, and nonmedical prescription use remains one of the most common forms of illicit substance abuse among young adults, second only to cannabis use (Substance Abuse and Mental Health Services Administration [SAMHSA], 2012). Unlike many other illicit substances, prescription drugs are unique in that they are made with an established medical purpose yet abused to the point of harm -- the opposite of their intended effect.
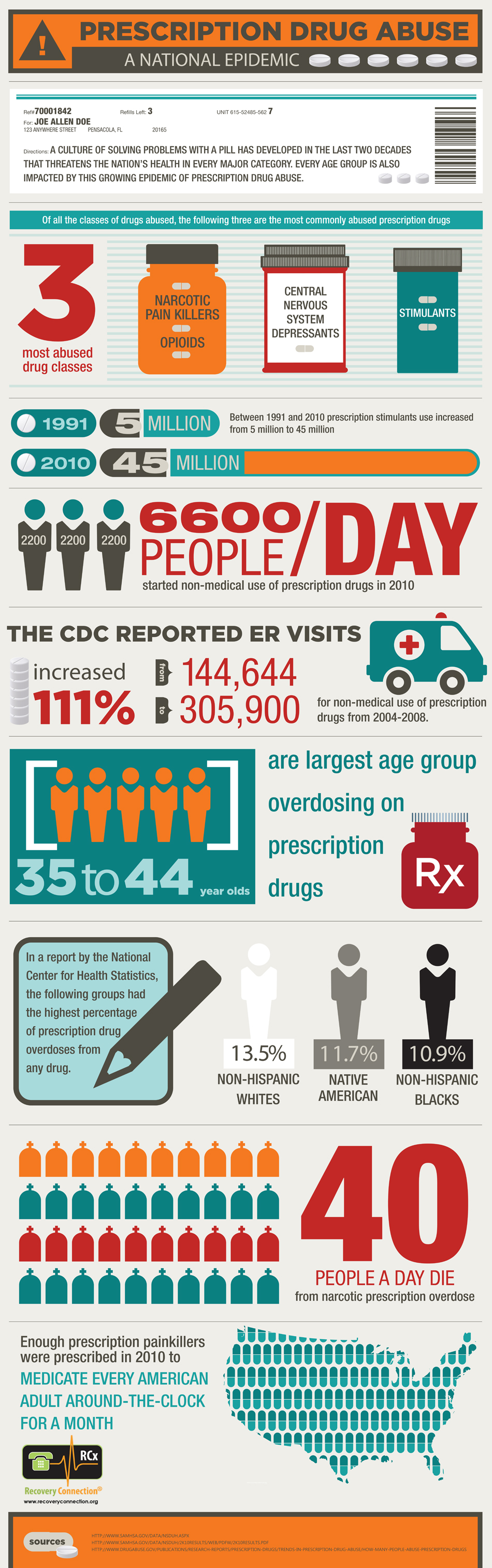
55% of abusers get their prescription drugs from friends or relatives. Meanwhile, a small number of doctors are responsible for writing large numbers of prescriptions. In an Oregon program, it was found that the top 8.1% of providers wrote 79% of all Schedule II-IV prescriptions.
Far from the shadowy worlds of heroin smuggling, cocaine dealing, and methamphetamine cooking, prescription drugs have become increasingly ubiquitous and blatant. In the year 2001 alone, Purdue Pharma L.P. spent two hundred million dollars marketing its drug OxyContin (Zee, 2009). Despite large public attention to the more nefarious seeming drugs (heroin, cocaine, meth, etc.), pharmaceutical drugs accounted for 58% of all drug overdoses in 2010; four times greater than cocaine and heroin combined (Jones, Mack & Paulozzi, 2013). Apart from the loss of life, prescription drug abuse incurs a monetary cost: pharmaceutical drugs cost health insurers up to $72.5 billion per year in drug diversion (Mahon, 2007), create $8 billion in criminal justice costs, and result in $42 billion in lost productivity (United States General Accounting Office [USGAO], 2002).
 Click image to enlarge full infographic.
Click image to enlarge full infographic.
The burden of prescription drug abuse is obvious, but what policies can be put into place to curb the rates or addiction, abuse, and overdose? With an issue as widespread and entrenched as nonmedical prescription drug abuse, it will likely take a long-term approach with an array of policies including Prescription Drug Monitoring Programs (PDMPs), substance abuse treatment (both behavioral and pharmacologic), “Good Samaritan” laws that grant legal immunity to people reporting an overdose, and public education on the issue. Of these tactics, PDMPs have been the most actively pursued by states in the last decade.
In general terms, a prescription drug monitoring program is an electronic database: a network to track the provision of drugs to patients. More specifically, a PDMP looks something like an automated evidence collecting system. This system tracks drug users and abusers, thereby giving prescribers and pharmacies access to a host of pertinent information they would lack otherwise. A doctor with an effective PDMP has an entire list of whatever medications their patient has been prescribed, when they were prescribed, who prescribed them, and when they were last filled. This information can aid the clinician in making the best possible medical decision, and lower rates of prescription drug misuse.
These PDMPs vary widely between states. For example, discrepancies exist in the type of information each system collects, the qualifications needed to access the information, and the enforcement policies in place to act on the information. As evidence of a difference between PDMPs, only 16 states require enrollment and participation by drug prescribers and dispensers; the rest are voluntary, so clinicians and pharmacists have the option to disregard PDMP information (USGAO, 2002). Differences in PDMPs thus create the potential for variation in program efficacy.
This paper begins by outlining the causes of nonmedical prescription drug use and then provides a summary of state PDMP adoption. From there, it makes the case for unsolicited reporting as a mechanism to attract attention to the program and automatically report doctor shoppers and pill mills. Ultimately I argue for widespread adoption of a cross state information exchange that would improve our ability to catch doctor shoppers that cross state lines in addition to short data collection intervals to maximize actionable information available to both clinicians and dispensers.
While PDMPs can be helpful in many situations, such as when elderly patients forget the last time they filled their blood pressure prescriptions, PDMPs may have their most significant benefit in situations involving substance abuse. According to a survey by SAMHSA (2013), 4.6% of Americans over the age of 12 used prescription pain relievers for nonmedical use between 2010 and 2012. In total, more than 20 million Americans have taken pain relievers for nonmedical purposes since 2002. Nonmedical abuse is defined as the use of drugs without a prescription or use that occurred simply for the experience or feeling the drug causes (SAMHSA, 2013).
These high rates can be attributed, in large part, to the pharmacological mechanism of the pain medications. Painkillers target receptors in the brain to reduce pain levels, with a common side effect being the feeling of euphoria (Centers for Disease Control and Prevention [CDC], 2013a). Opioids, for example, target the same brain receptors as heroin. Individuals prone to addiction may experience dependence, the gradual need for higher doses to produce an effect, as well as addiction. For these people, pain medication becomes more than a remedy to physical ailment, it becomes a means towards a high.
Considering that many nonmedical users are pursuing a high, the question can be raised: how are so many people getting their hands on addictive prescriptions in the first place? Part of the issue stems from prescribers’ willingness to give out pain medications. Throughout the 1980s and 1990s doctors were taught to think of pain as the “fifth vital sign.” Studies of today’s most prevalent pain medications claimed that they pose a minimal risk of addiction; in fact, as recent as 2001, Purdue Pharma widely distributed brochures asserting that less than 1% of patients taking opioids become addicted (Seppala & Rose, 2010). This has been proven catastrophically false (Boscarino et al., 2010). Even so, the prescription rate of opioids, for patients complaining of pain, has risen from 11.3 to 19.6% between 2000 and 2010 (Korff, 2013). Somewhere near 219 million opioid prescriptions were made in 2011 alone (Whoriskey, 2012).
Somewhat surprisingly, 55% of abusers get their prescription drugs from friends or relatives; in total, more than three out of four abusers get them from someone else through a practice known as diversion (SAMHSA, 2011). This should be viewed as an oversupply since many patients for whom prescriptions are written, are not actually taking them. More troubling still, recent data indicates that a relatively small number of doctors are responsible for a large volume of prescriptions: Oregon’s Prescription Drug Monitoring Program (2012) found that the top 8.1% of providers wrote 79% of all Schedule II-IV prescriptions.
When prescribing practices become extreme, the physician or clinic can become known as a pill mill. Pill mills represent a significant roadblock in the way of curbing prescription drug abuse. A pill mill is, according to Cichon (2013): “a doctor’s office, clinic, or healthcare facility that routinely conspires in the prescribing and/or dispensing of controlled substances outside the scope of the prevailing standards of medical practice.” These operations are lucrative for the less scrupulous of doctors; those willing to leverage their medical licensure to sell prescriptions.
On the other side of the issue is doctor shopping. The more frequent prescription drug abusers are willing to go to great ends in order to get their hands on the next prescription, despite nearly every state having its own form of anti-doctor shopping laws (CDC, 2012). Doctor shopping is not always a reference to searching with malign intentions, but searching for clinicians willing to write prescriptions for pain relievers is an increasingly common practice as abuse rates rise (McDonald & Carlson, 2013). In a study based upon 2008 data, McDonald and Carlson (2013) found that roughly 3% of opioid purchasers obtained their prescriptions from between 5 and 9 prescribers, 0.35% obtained them from 10 to 19 prescribers, and 0.04% obtained them from more than 19. In cases such as these, the extent of the issue is made clear. Any prescription seeker capable of getting painkillers from more than 19 doctors poses a real threat to both themselves and anyone to whom they may peddle the drugs.Continued on Next Page »
Boscarino, J.A., Rukstalis, M., Hoffman, S.N., Han, J.J., Erlich, P.M., Gerhard, G.S., & Stewart, W.F. (2010). Risk factors for drug dependence among out-patients on opioid therapy in a large US health-care system. Addiction, 105, 1776–1782. doi: 10.1111/j.1360-0443.2010.03052.x
Budnitz, D.S., Pollock, D.A., Weidenbach, K.N., Mendelsohn, A.B., Schroeder, T.J., & Annest, J.L. (2006). National Surveillance of Emergency Department Visits for Outpatient Adverse Drug Events. JAMA. 296(15), 1858-1866. doi: 10.1001/jama.296.15.1858
Center for Disease Control and Prevention. (2012, July). Law: Doctor Shopping. Retrieved from http://www.cdc.gov/homeandrecreationalsafety/Poisoning/laws/dr_shopping.html
Center for Disease Control and Prevention. (2013a, July ). Policy Impact: Prescription Painkiller Overdoses. Retrieved from http://www.cdc.gov/homeandrecreationalsafety/rxbrief/
Center for Disease Control and Prevention. (2013b, December). New CDC Vital Signs: Prescription Painkiller Epidemic Among Women. Retrieved from http://www.cdc.gov/media/dpk/2013/dpk-Prescription%20drug%20overdose.html
Cichon, C. (2013). Pill Mills and Pain Management: Legislation and Enforcement [Presentation slides]. Retrieved from http://www.une.edu/com/cme/upload/Pill-Mills-and-Pain-Management-Pain-Week-2013cichon.pdf
Clark, T., Eadie, J., Kreiner, P., & Strickler, G. (2012). Prescription Drug Monitoring Programs: An Assessment of the Evidence for Best Practices. Retrieved from http://www.pewhealth.org/uploadedFiles/PHG/Content_Level_Pages/Reports/PDMP%20Update%201-31-2013.pdf
Dormuth, C.R., Miller, T.A., Huang, A., Mamdani, M.M., & Juurlink, D.N. (2012). Effect of a centralized prescription network on inappropriate prescriptions for opioid analgesics and benzodiazepines. CMAJ, 184, 852–56. doi: 10.1503/cmaj.120465
Doland, P. (2012, September 20). Study quantifies drug monitoring database’s effect on opioid prescriptions. Amednews. Retrieved from http://www.amednews.com/article/20120920/business/309209997/8/
French, M. (2014, February 11). Prescription drug database gets first-round approval in Missouri House. St. Louis Post-Dispatch. Retrieved from http://www.stltoday.com/news/local/govt-and-politics/political-fix/prescription-drug-database-gets-first-round-approval-in-missouri-house/article_8623bf88-5c39-53af-a9fc-5743107c9a40.html
Hopkins, D. (2012, July). Prescription Drug Monitoring Program Interstate Data Sharing [Presentation slides]. Retrieved from http://www.ncja.org/sites/default/files/documents/Hopkins_Prescription_Drug_Monitoring_Program.pdf
IEEE Computer Society. (2000). IEEE Recommended Practice for Architectural Description of Software-Intensive Systems: IEEE Std 1472000. Retrieved from http://www.ibm.com/developerworks/rational/library/feb06/eeles/
Jones, C.M., Mack, K.A., & Paulozzi, L.J. (2013). Pharmaceutical Overdose Deaths, United States, 2010. JAMA, 309(7), 657-659. doi:10.1001/jama.2013.272
Lear, M. (2011, February 11). House gives initial approval to prescription drug monitoring program. MissouriNet. Retrieved from http://www.missourinet.com/2014/02/11/house-gives-initial-approval-to-prescription-drug-monitoring-program/
Paulozzi, L.J., Jones, C.M., Mack, K.A., & Rudd, R.A. (2011). Vital Signs: Overdoses of Prescription Opioid Pain Relievers — United States, 1999–2008. Morbidity and Mortality Weekly Report, 60(43), 1487-1492, Retrieved from http://www.cdc.gov/mmwr/pdf/wk/mm6043.pdf
Lammers, E., Adler-Milstein, J., & Kocher, K. (2013). Does Health Information Exchange Reduce Redundant Imaging? Evidence From Emergency Departments. Medical Care, 1, doi: 10.1097/MLR.0000000000000067
Mahon, W. (2007). Prescription for Peril: How Insurance Fraud Finances Theft and Abuse of Addictive Prescription Drugs. Coalition Against Insurance Fraud. Retrieved from http://www.insurancefraud.org/downloads/drugDiversion.pdf
McDonald, C. & Carlson, E. (2013). Estimating the Prevalence of Opioid Diversion by “Doctor Shoppers” in the United States. PLoS ONE. 8(7), doi:10.1371/journal.pone.0069241
Michael, B. (2013). Prescription Drug Monitoring Program [Presentation slides]. Retrieved from http://adaa.dhmh.maryland.gov/Documents/SDAACWeb/Minutes/PrescriptionDrugMonitoringProgram_PDMP.ppt
National Association of Boards of Pharmacy. (2012, May 23). NABP PMP InterConnect Committed to PMIX Architecture Compliance; BJA to Immediately Release Funding for PMP InterConnect Participants. Retrieved from http://www.nabp.net/news/nabp-pmp-interconnect-committed-to-pmix-architecture-compliance-bja-to-immediately-release-funding-for-pmp-interconnect-participants
Oklahoma Department of Mental Health and Substance Abuse Services. (n.d.) Fact Sheet on Prescription Drug Abuse, Misuse and Consequences. Retrieved from Oklahoma Department of Mental Health and Substance Abuse Services website: http://ok.gov/odmhsas/documents/PR%20RxAbuse-FactSheet.pdf
Oregon Prescription Drug Monitoring Program Center for Prevention and Health Promotion. (2012). Prescription Controlled Substance Dispensing in Oregon: October 1, 2011 – March 31, 2012. Statewide Data Report. Retrieved from Oregon PDMP website: http://www.orpdmp.com/orpdmpfiles/PDF_Files/Reports/Statewide_10.01.11_to_03.31.12.pdf
PDMP Center of Excellence. (2011). Trends in Wyoming PMP Prescription History Reporting: Evidence for a Decrease in Doctor Shopping? Retrieved from http://www.pdmpexcellence.org/sites/all/pdfs/NFF_wyoming_rev_11_16_10.pdf
PDMP Center of Excellence. (2014). Options for Unsolicited Reporting. Retrieved from http://www.pdmpexcellence.org/sites/all/pdfs/Brandeis_COE_Guidance_on_Unsolicited_Reporting_final.pdf
PDMP Training and Technical Assistance Center. (n.d.) PDMP Data Collection Interval. Retrieved from PMDP Training and Technical Assistance Center website: http://www.pdmpassist.org/content/pdmp-data-collection-frequency?order=field_frequency_data_collected_value&sort=asc
Reifler, L.M., Droz, D., Bailey, J.E., Schnoll, S.H., Fant, R., Dart, R.C., & Bartelson, B.B. (2012). Do Prescription Monitoring Programs Impact State Trends in Opioid Abuse/Misuse? Pain Medicine, 13(434–442). doi: 10.1111/j.1526-4637.2012.01327.x
Seppala, D., & Rose, M. (2010). The History of Opioids. In Prescription Painkillers: History, Pharmacology, and Treatment (pg. 17-28). Center City, MN: Hazelden.
Simeone, R. & Holland, L. (2006). An Evaluation of Prescription Drug Monitoring Programs. Retrieved from National Criminal Justice Reference Service Website: https://www.ncjrs.gov/app/publications/abstract.aspx?ID=238896
Substance Abuse and Mental Health Services Administration. (2011). Results from the 2010 National Survey on Drug Use and Health: Summary of National Findings, NSDUH Series H-41, HHS Publication, 11(4658), Retrieved from http://www.samhsa.gov/data/NSDUH/2k10NSDUH/2k10Results.pdf
Substance Abuse and Mental Health Services Administration. (2012). Results from the 2011 National Survey on Drug Use and Health: Summary of National Findings. Retrieved from SAMHSA website: http://www.samhsa.gov/data/nsduh/2k11results/nsduhresults2011.pdf
Substance Abuse and Mental Health Services Administration. (2013, January). The NSDUH Report: State Estimates of Nonmedical Use of Prescription Pain Relievers. Retrieved from SAMHSA website: http://www.samhsa.gov/data/2k12/NSDUH115/sr115-nonmedical-use-pain-relievers.htm
The American Society for Automation in Pharmacy. (2014, April 13). ASAP News. Retrieved from ASAP website: http://www.asapnet.org/home.html
United States Department of Justice, Bureau of Justice Assistance. (n.d.) Prescription Drug Monitoring Programs: Critical Information Sharing Enabled by National Standards. Retrieved from https://www.bja.gov/Programs/PMIXArchitecture.pdf
United States General Accounting Office. (2002). Prescription Drugs State Monitoring Programs Provide Useful Tool to Reduce Diversion. Retrieved from http://www.gao.gov/assets/240/234687.pdf
Vogt, D. (2012). ‘Real-Time Reporting’ Paving the Road and Avoiding and Potholes [Presentation slides]. Retrieved from PDMP Center of Excellence website: http://www.pdmpexcellence.org/sites/all/pdfs/pmp_real_time_national.pd
Vogt, D. (2013). A Foundation for Choice: PMIX Architecture. [Presentation slides]. Retrieved from ASAP website: http://www.asapnet.org/files/January2013/ASAPJan13_Pres02_Vogt.pdf
Von Korff, R. (2013). Health Care for Chronic Pain: Overuse, Underuse, and Treatment Needs: Commentary on: Chronic Pain and Health Services Utilization-Is There Overuse of Diagnostic Tests and Inequalities in Nonpharmacologic Methods Utilization? Medical Care. 51(10), 857-858. doi: 10.1097/MLR.0b013e3182a53db3
Weisberg, A., Strub, R., & Garcia, C. (1983). Episodic Loss of Conscious. In Essentials of Clinical Neurology (pp. 8-1 to 8-13). Baltimore: University Park. Retrieved from: http://tulane.edu/som/departments/neurology/programs/clerkship/upload/wch8.pdf
White, A.G., Birnbaum, H.G., Schiller, M., Tang, J., & Katz, N.P. (2009). Analytic Models to Identify Patients at Risk for Prescription Opioid Abuse. American Journal for Managed Care, 15, 897-906. Retrieved from: http://www.ajmc.com/publications/issue/2009/2009-12-vol15-n12/ajmc_09dec_white_897to906/1#sthash.Xi3jWake.dpuf
Whoriskey, P. (2012, December 30). Rising painkiller addiction shows damage from drugmakers’ role in shaping medical opinion. The Washington Post. Retrieved from http://www.washingtonpost.com/business/economy/2012/12/30/014205a6-4bc3-11e2-b709-667035ff9029_story.html
Zee, A. (2009). The Promotion and Marketing of OxyContin: Commercial Triumph, Public Health Tragedy. American Journal of Public Health, 99(2), 221-227. doi: 10.2105/AJPH.2007.131714