Intergenerational Intimate Partner Violence: Pathways of Genetic and Environmental Interactions
By
2020, Vol. 12 No. 09 | pg. 1/1
IN THIS ARTICLE
KEYWORDS
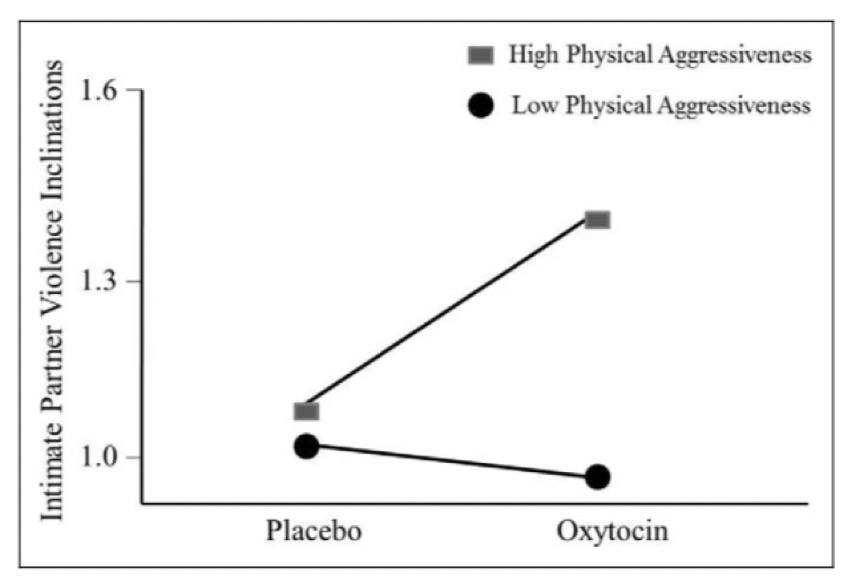
AbstractIntimate partner violence (IPV) is a serious public health issue that results in social, psychological, emotional, and physical consequences. Although interventions may be continuously designed to combat this problem, IPV must first be understood in an intergenerational perspective before effective programs can be put into place. Intimate partner violence is historically viewed as a social and private phenomenon, tinged with shame and stigma. Existing literature on this issue predominantly focuses on the social environment, leaning towards theories that put blame on the social environment the victims are bound to. IPV however, is an intergenerational cycle; genetic and biological factors cannot be ignored in IPV perpetration and victimization. Because it is a cycle, the beginning of the pathway of violence may be hard to target. This paper seeks to identify the major beginning points of the various pathways that lead to intimate violence perpetration and victimization by highlighting the social environmental factors, as well as the biological factors and assesses whether one kind of factor could be the sole indicator of IPV without the other. Intimate partner violence (IPV) is a serious public health problem that leads to grave biological and psychological consequences for victims and families in diverse ways. Based on the Center for Disease Control (CDC) definition, intimate partner violence encompasses “physical violence, sexual violence, stalking, or psychological aggression (including coercive acts) by a current or former intimate partner, whether or not the partner is a spouse.”1 This form of violence in society is underreported by victims for various reasons that could range from not wanting to be publicly shamed to not wanting to report someone they love. A troubling but consistent finding in the existing research is that IPV tends to “run in the family.”2 Families are usually private, which makes it more difficult for society to provide effective interventions for victims of IPV when the perpetrator is their husband or their wife. To create beneficial interventions for these victims, the nature of the intergenerational cycle of IPV must be understood. The purpose of this paper is to identify the starting factors that activate the cascade of conditions that lead to or continue the intergenerational IPV cycle and to argue that neither the social environmental factors nor the biological factors can explain this phenomenon alone; the combination of the gene and environment interactions show the most predisposition for IPV perpetration and victimization. First, I will explain the dominating literature about intergenerational IPV, which focuses on social theories, such as the Social Learning Theory and the Attachment Theory, which purely attribute intergenerational IPV perpetration and victimization later in life to environmental factors. For this type of framework, the pathway to IPV perpetration or victimization begins with early exposure to violence. However, biologically related families also share genes, so biological factors, such as cognitive functions, neurochemical functions, psychophysiological functions, and genes must also be taken into account. For the biological framework, the pathway to IPV perpetration or victimization of the individual begins with a gene or a physiological condition. Finally, I will discuss the interactions between genes and the environment and their significant influences on intergenerational IPV pathways.Social Environmental FactorsSocial theories that focus on the social environment the individual is surrounded with is crucial to understand because of humans are social beings; the social aspect of relationships cannot be taken away from the progression of IPV. The pathway to IPV perpetration or victimization based on the social environmental theories begins with early exposure to violence. It is important to note, however, that these theories are insufficient for the greater understanding of intergenerational IPV. Social Learning TheoryThe Social Learning Theory is usually used to explain “the cycle of intergenerational violence, suggesting that children typically model the aggressive behaviors of same-gender role models.”3 The aggressive behaviors could either be intimate partner violence committed by the parents, which the children witness, or child abuse committed by the parent, which the children experience. In childhood conditions where a parent is committing IPV, the individual is more likely to model that behavior, especially in their disagreements with loved ones later in life.2 In fact, “the witnessing of interparental violence doubles one’s odds of perpetrating intimate partner violence.”3 Based on the Social Learning Theory, boys who witness their father committing violence against women should have a higher risk for becoming perpetrators in their own relationships, while girls who witness their father committing violence against women should have a higher risk for becoming IPV victims in their own relationships. In this study, however, it was shown that the prediction about the boys was found to be true, but the association between opposite-gender perpetration and victimization for girls was not significant at conventional levels.4 In the case that the child is abused by his/her parents, the odds of him/her perpetrating intimate partner violence increases 1.5 times.3 The Social Learning Theory has received many criticisms about how it neglects to consider how genetic factors could play a role in intergenerational IPV. This gap in the theory can be pointed out by the effect of witnessing bidirectional IPV. Bidirectional IPV refers to the victim-offender overlap, which is the finding that “perpetrators of aggressive behavior are disproportionately likely to also be victims of aggressive behavior for IPV.”5 On the one hand, Social Learning Theory can argue that children who witness bidirectional IPV will have increased risk for combined perpetration and victimization of IPV in the future.4 On the other hand, the genetic similarity of family members could also contribute to the increased risk. Another notable deficiency of the Social Learning Theory is that it is over-simplistic due to the fact that the transmission of violence is not 100%.3 Because this theory alone cannot completely predict who will perpetrate IPV in the future, it cannot be enough to explain intergenerational IPV on its own. Attachment TheoryThe Attachment Theory suggests that individual variation in attachment orientations influence (and are influenced by) cognitive and behavioral responses in romantic relationship.5 The variation in attachment stems from differences in proximity, dependency, expectations held for the significant other. For example, attachment anxiety, which is characterized by hyperactivation of romantic attachment and overdependence on a partner for stability and security, is a predictor for IPV perpetration and victimization because the individuals with this condition tend to display coercive or controlling behaviors to evoke investment and attachment from their partner.5 The Attachment Theory could also be applied in combination with the Social Learning Theory. Individuals with a history of child abuse are more likely to treat loved ones in hostile ways. Applying the Social Learning Theory, the early “parent-child attachment relationship was a prototype for that child’s later relationships.”3 Because the child’s attachment orientation in his future relationships replicates the attachment orientation he/she witnessed and experienced from an early age, he/she may be more likely to become a perpetrator of IPV, continuing the intergenerational cycle. Biological FactorsThe biological factors that predict or increase risk for IPV perpetration or victimization are important to recognize because these traits can be passed down to offspring, contributing to the transgenerational nature of IPV. In this framework, the pathway to IPV perpetration or victimization of the individual begins with a cognitive, neurochemical, or physiological condition. However, the individual’s biological factors without considering the environment cannot explain the entirety of transgenerational IPV, which must take a more multifaceted perspective. Cognitive FunctionDiminished cognitive functioning is significant for determining predisposition for IPV perpetration. High levels of alcohol consumption has been found to decrease cognitive functioning, such as executive functions, and increase aggression. According to the study “Differential Cognitive Profiles of Intimate Partner Violence Perpetrators Based on Alcoholic Consumption,” IPV perpetrators that consumed high levels of alcohol had “slower processing speed and significantly more impairment sin attentional set-shifting or switch attention, working and long-term memory, cognitive flexibility, planning, decision-making, emotional decoding skills, and perspective taking” than the controls.6 In addition, the relationship between alcohol consumption and violence perpetration is significant due to increased aggression. These factors combined increase the likelihood of the perpetrator committing violence after drinking alcohol. Another cause of diminished cognitive functioning is head injury. Based on “Biological Correlates of Intimate Partner Violence Perpetration,” having a prior head injury, when comparing abusers with non-abusers, appeared to increase the likelihood of being an abuser six-fold no matter the severity of the injury.7 Similar to the effects of alcohol consumption, head injuries seem to also impair cognitive functions. For example, IPV perpetrators with head injuries seemed to perform poorly on tests of executive functioning, attention, learning and memory, and verbal ability.7 Both alcohol consumption and head injuries have serious effects on frontal lobe behavior, increases aggression, and increases the likelihood of becoming an IPV perpetrator. Neurochemical FunctionIn the existing literature, neurochemical functions have also been found to influence the likelihood of IPV perpetration. For example, high levels of testosterone, the main male sex hormone, is associated with high levels of aggression.7 High levels of aggression could be a predisposition for higher likelihood for IPV perpetration due to short tempers and impulsivity. An interesting finding showed that “complementary levels of testosterone between partners, such that one partner is high in testosterone and the other partner is low testosterone, were associated with less hostility and aggression; however, partners with similar levels of testosterone (either both high or both low) had the most destructive levels of psychological and physical aggression.7 This study showed that the levels of testosterone in the individual partners in a relationship influenced the likelihood of IPV perpetration. Another example is that low levels of serotonin can lead to high levels of aggression, which can have similar results in IPV perpetration. IPV perpetrators without the influence of alcohol were significantly associated with low levels of serotonin and high levels of aggression.7 Oxytocin is also associated with IPV inclinations. This hormone is a nonapeptide that has both peripheral and central functions, and trait physical aggressiveness.13 In the study “When the Love Hormone Leads to Violence: Oxytocin Increases Intimate Partner Violence Inclinations Among High Trait Aggressive People,” oxytocin was found to increase IPV inclinations but only for participants who were already prone to physical aggression.13 These three types of hormones have been predictors of IPV in the existing research. Psychophysiological Function
Figure 1. Physical Aggression Interacts with Oxytocin Condition13 Psychophysiological factors can also be a predictor for IPV perpetration. Low resting heart rate is associated with physical psychological aggression, more antisocial personality traits, and greater general violent behavior, especially for male-to-female violence.7 Heart rate can be used as a measurement for determining IPV perpetration. In fact, “low resting heart rate is a better predictor of psychopathy and interpersonal violence than HR reactivity to interpersonal conflict.”7 Another psychophysiological factor is skin conductance, which is used to measure emotional arousal. Low skin conductance, in particular, has been associated with antisocial traits in highly violent adult men.14 Gene x Environment InteractionIntergenerational IPV is heavily influenced by genetics. According to “Indicators of Domestic/Intimate Partner Violence Are Structured by Genetic and Nonshared Environmental Influences,” “genetic influences are often the primary reason family members resemble one another on any trait.”2 Although social theories and biological reasonings could be used to explain risk factors and certain predispositions for IPV, they alone cannot complete the full picture of how intergenerational IPV is able to take place without genetics. In this study, genetic factors were found to explain 50% of the variance in each of the three IPV indicators, hitting partner, injuring partner, and forcing sexual activity, which is accounts for the majority of the variance.2 However, nonshared environment explained the remainder of the variance in the three indicators, which leads to the important consideration of gene-environment interactions. Gene-environment interactions have the potential to close the gap of understanding in intergenerational IPV. According to “Intergenerational Transmission of Intimate Partner Violence,” “genetic factors play a larger role than environmental factors, but when both are combined, they increase risk for criminality exponentially.”3 In the next sections, I will explain some gene-environment interactions that have been shown to lead to perpetration and victimization of IPV and could account for the intergenerational transmission of IPV risk. Prenatal Gene x IPV InteractionPhysical intimate partner violence committed during a woman’s pregnancy can have devastatingly increase the risk of their unborn child committing IPV later in life. The pathway begins with the physical IPV and the pregnant woman’s victimization, and this leads to a genetic shift in the unborn baby that can have a poor impact on their general health. In the study “Prenatal Intimate Partner Violence Exposure Predicts Infant Biobehavioral Regulation: Moderation by the Brain-Derived Neurotrophic Factor (BDNF) Gene,” the BDNF gene has been found to contribute to stress vulnerability and susceptibility to negative effects of early adverse experiences; in short, this gene interacted with prenatal stress.8 The study focused on the BDNF gene and physical IPV in utero to determine whether the infants had increased cortisol response after birth. The results showed that there was “significant interaction for total IPV during pregnancy and BDNF on infant cortisol mobilization.”8 Cortisol release from the hypothalamic-pituitary-adrenal (HPA) axis is associated with high stress response. Children “who are reactive to stress (for example, as measured by cortisol output) early in life experience worse outcomes when raised in adversity than non-reactive children” because they are more prone to maladaptive behaviors later in life.9 High levels of cortisol is linked to high levels of aggression, which can predispose individuals to IPV perpetration. Another gene that reacts with in utero IPV is the glucocorticoid receptor (GR) gene. Like the BDNF gene, “the human GR gene is also affected by aversive social environments, “but this gene expresses the interaction through methylation .10 This study focused on the methylation status of the mother and the umbilical cord blood during a pregnancy experienced with IPV and found that “maternal gestational IPV is associated with methylation of exon 1F in the GR promoter of the offspring, which is hence a transgenerational effect that may exert a lifelong influence on HPA-axis regulation in these individuals, which can increase cortisol stress responses and psychopathology of offspring later in life”10 IPV experienced during pregnancy is a clear example of how gene-environment expression can lead to intergenerational IPV. The gene changes expression in the unborn offspring specifically due to IPV experienced by the pregnant mother perpetuates the cycle and genetically predisposes the child to higher risk to perpetrate IPV. Gene x Childhood Abuse Interaction
Figure 2. Cortisol Responder Status Based on Pregnancy IPV Level8 Even after birth, genes can still change expression of the child and increase their risk of higher levels of aggression and their risk for IPV perpetration later in life. A good example of this is the monamine oxidase A (MAOA) gene. Low levels of MAOA has been associated with impulsive behavior and conduct disorder.7 Furthermore, low levels of MAOA in combination with child maltreatment “developed conduct disorder, antisocial personality, and violent criminality in adulthood than maltreated children with a high-activity MAOA genotype.”11 These conditions could increase the risk of IPV perpetration or victimization later in life due to higher levels of aggression. The glucocorticoid receptor (GR) gene mentioned earlier was found to also have a gene-environment interaction through childhood abuse, even after the prenatal stage, which could lead to increased methylation, activating the cascade of conditions that can lead to higher risk of IPV perpetration later in life.10 This is just another example of how gene-environment interaction exhibits the transgenerational aspect of IPV. Gene x Violence Exposure InteractionAnother gene-environment interaction worth noting is the relationship between violence exposure at an early age and dopamine receptor genes. Dopamine is a neurotransmitter with significant influence on motivation and learning in an individual.12 In “Interactions of Adolescent Social Experiences and Dopamine Genes to Predict Physical Intimate Partner Violence Perpetration,” interactions between three dopamine gene alleles that were previously associated with violent behavior were found not to have an independent association with IPV perpetration.12 Because there is existing research that dopamine genes are associated with violent behavior, more research should be done to either recreate the conclusions or confirm this study’s results that the dopamine risk alleles do not have an association with IPV perpetration later in life. ConclusionIntimate partner violence seems to be a public health problem with no complete solutions because of the intergenerational nature of its transmission. However, there seems to be hope for new interventions if further research in the right departments are progressed and implemented. In this paper, I reviewed the social environmental factors, such as the Social Learning Theory and the Attachment Theory, which both focus on the social environment of the individual that predisposes the individual to have a higher risk for IPV victimization or perpetration. These factors begin at the early exposure of violence in childhood that leads to IPV later in life. Whether the early exposure of violence is witnessed or experienced, this exposure to violence increases the likelihood of perpetration and victimization.3 Then, I discussed the biological factors that can determine, measure, or predict IPV perpetration, such as diminished cognitive functions, varied neurochemical functions, and specific psychophysiological function, characterized the pathway to IPV perpetration for individuals. Both frameworks are useful but must be combined to understand the transgenerational nature of IPV. Frameworks using gene-environment interactions seemed to be the best interdisciplinary method to discuss IPV transmission in families and to move forward with in future research. In gene-environment interactions, IPV experienced prenatally or witnessed in childhood seemed to change genes in individuals that can perpetuate the transmission of IPV risk in the cycle. References1. Miller E, McCaw B. Intimate Partner Violence. The New England Journal of Medicine. 2019;380(9): 850-857. 2. Barnes JC, TenEyck M, Boutwell BB, Beaver KM. Indicators of domestic/intimate partner violence are structured by genetic and nonshared environmental influences. Journal of Psychiatric Research. 2013;47: 371-376. 3. Hines DA, Saudino KJ. Intergenerational Transmission of Intimate Partner Violence: A Behavioral Genetic Perspective. Trauma, Violence, & Abuse. 2002;3(3): 210-225. 4. Forke CM, Myers RK, Fein JA, Catallozzi M, Localio AR, Wiebe DJ, Grisso JA. Witnessing intimate partner violence as a child: How boys and girls model their parents’ behaviors in adolescence. Child Abuse & Neglect. 2018;84: 241-252. 5. Barbaro N, Boutwell BB, Shackelford TK. Associations between attachment anxiety and intimate partner violence perpetration and victimization: Consideration of genetic covariation. Personality and Individual Differences. 2019;147: 332-343. 6. Vitoria-Estruch S, Romero-Martínez A, Lila M, Moya-Albiol L. Differential Cognitive Profiles of Intimate Partner Violence Perpetrators Based on Alcohol Consumption. Alcohol. 2018;70: 61-71. 7. Pinto LA, Sullivan EL, Rosenbaum A, Wyngarden N, Umhau JC, Miller MW, Taft CT. Biological Correlates of Intimate Partner Violence Perpetration. Aggression and Violent Behavior. 2010;15: 387-398. 8. Martinez-Torteya C, Figge CJ, Gilchrist MA, Muzik M, King AP, Sorenson M. Prenatal Intimate partner violence exposure predicts infant biobehavioral regulation: moderation by the brain-derived neurotrophic factor (BDNF) gene. Development and Psychopathology. 2018;30: 1009-1021. 9. Bair-Merrit MH, Voegtline K, Ghazarian SR, Granger DA, Blair C, Family Life Project Investigators, Johnson SB. Maternal intimate partner violence exposure, child cortisol reactivity and child asthma. Child Abuse & Neglect. 2015;48: 50-57. 10. Radtke KM, Ruf M, Gunter HM, Dohrmann K, Schauer M, Meyer A, Elbert T. Transgenerational Impact of intimate partner violence on methylation in the promoter of the glucocorticoid receptor. Translational Psychology. 2011;21: 1-6. 11. Kim-Cohen J, Caspi A, Taylor A, Williams B, Newcombe R, Craig IW, Moffitt TE. MAOA, maltreatment, and gene-environment interaction predicting children's mental health: new evidence and a meta-analysis. Molecular Psychiatry. 2006;11(10): 903-913. 12. Schwab-Reese LM, Parker EA, Peek-Asa C. Interactions of adolescent social experiences and dopamine genes to predict physical intimate partner violence perpetration. PLoS ONE. 2017;12(3): 1-12. 13. DeWall CN, Gillath O, Pressman SD, Black LL, Bartz JA, Moskovitz J, Stetler DA. When the Love Hormone Leads to Violence: Oxytocin Increases Intimate Partner Violence Inclinations Among High Trait Aggressive People. Social Psychological and Personality Science. 2014;5(6): 691-697. 14. Romero-Martínez A, Lila M, Williams RK, Gonzalez-Bono E, Moya-Albiol L. Skin conductance rises in preparation and recovery to psychosocial stress and its relationship with impulsivity and testosterone in intimate partner violence perpetrators. International Journal of Psychophysiology. 2013;90(3): 329-333. 
From the Inquiries Journal Blog   Related Reading Monthly Newsletter SignupThe newsletter highlights recent selections from the journal and useful tips from our blog. Suggested Reading from Inquiries Journal
Inquiries Journal provides undergraduate and graduate students around the world a platform for the wide dissemination of academic work over a range of core disciplines. Representing the work of students from hundreds of institutions around the globe, Inquiries Journal's large database of academic articles is completely free. Learn more | Blog | Submit Follow IJ
Latest in Psychology |