The HIV/AIDS Epidemic in the Deep South
Clocks and Clouds
2012, Vol. 1 No. 1 | pg. 1/1
Abstract
This paper examines explanations for the current HIV/AIDS epidemic in the Deep South United States. The first set of explanations is categorized as social determinants of health and includes social and economic factors that influence public health care such as poverty rates, high school graduation rates, and existing health infrastructure in the region. The second set of explanations examines the influence of less visible barriers to health care, and includes studies related to shared communal narratives of conspiracy theories and stigma. The paper employs a quantitative analysis of social and economic data from four states, Alabama, Mississippi, Oklahoma, and Ohio, to demonstrate that social and economic data alone cannot explain why the HIV/AIDS epidemic is growing so rapidly in the Deep South but not in other regions of the country. The results from the data analysis conclude that cultural factors, such as conspiracy theories and stigma, may carry greater explanatory power than what is generally assumed. This paper concludes with implications for future research into the impact of stigma and conspiracy theories on public health and the HIV/AIDS epidemic in the Deep South.
"Save yourself a transatlantic airline fare to a developing country. Just come to Mississippi...." – Craig Thompson, Director, Office of HIV/STD, Mississippi State Department of Health, interview with Human Rights Watch
Introduction
The HIV/AIDS epidemic in the United States started in 1981. After contracting HIV a person can go eight years before symptoms appear. This makes the HIV/AIDS virus particularly hard to track. Throughout the 1980s the HIV/AIDS virus spread mostly in the northeast and western areas of the country. That has since changed. Now HIV/AIDS rates are increasing most rapidly in the six states that make up the Deep South (Alabama, Georgia, Louisiana, Mississippi, North Carolina and South Carolina). From 2000 to 2003, the number of new reported AIDS cases increased 35.6% in the Deep South, and only 4.0% in other Southern states (Florida, Kentucky, Tennessee, Texas, West Virginia, and Virginia) and 5.2% nationally (Reif, Geonnotti, Whetten 2006, 971). This presents a challenge to public health policymakers. Given the advances in the development of antiretroviral drugs, surveillance methods, and stopping the spread of the disease in other parts of the country since 1981, what is responsible for the increase in HIV/AIDS rates in the Deep South?
The Deep South states share several common factors, in addition to their rising HIV/AIDS rates. These states share a common history of an agrarian economy based on plantations and slave labor. In addition, they have a 30% Black population compared to 12% nationally (McKinnon 2000). Nationally, African-Americans bear a disproportionate burden of 44% of HIV/AIDS cases, and this is especially true in the Deep South where 70% of the reported cases are African-Americans (Reif, Geonnotti, Whetten 2006, 971)
Identifying the barriers confronted by marginalized groups is essential for effective public health care. The rapid rate of the spread of HIV/AIDS creates an urgent need for more research into the factors explaining its increase. This paper will examine the role socio-economic and cultural barriers have in the rural Deep South's HIV/AIDS epidemic, and the need for greater research and attention to less visible communal narratives, what one might be tempted to called "cultural" factors. Both socio-economic and cultural approaches are important. However, cultural barriers are hard to quantify and consequently are often over looked.
It is important to understand what the word culture means. In past social science research cultural relativism has been used to advance the idea that because every culture is unique, the inequalities within that society must be respected as an inherent part of that culture. Poverty, inequality, and structural violence are confused as endemic parts of a different culture. "Culture difference is used to explain away assaults on dignity and suffering instead of focusing on the national and international mechanisms that [perpetuate inequality]" (Farmer 2005, 48). Culture when used in this paper refers to the intangible influence of commonly held ideas within a certain community.
Specifically, two commonly held ideas are examined within the African-American community: conspiracy theories and stigma. Conspiracy theories refer to beliefs within some parts of the African-American community that government programs, including medical programs, are purposefully designed to harm and repress African-Americans. Stigma refers to the perception of HIV/AIDS as a mark or sign of disgrace, or even a manifestation of sin for sexual misbehavior. These ideas, however, are very much linked to and caused by state and national actions. Conspiracy theories are the legacy of narratives within the Black community that are the result of distrust and fear caused by a history of violent and repressive actions taken by the state against its own people. Stigma persists because of a failure by state health institutions to recognize the need for addressing it through adequate public health education or outreach campaigns.
The paper will examine the question, what is causing the increase in HIV/AIDS rates in the Deep South? The paper's focus will be confined to the disease's spread in the last 10 years, when the sharp increase in HIV/AIDS rates in the Deep South was first reported. The paper builds on several decades' worth of literature on the structural barriers to health care in the Deep South. It also examines literature on imbedded conspiracy theories and stigma found in the Black community and their implications for HIV/AIDS.
Literature Review
A lot has been written about structural factors that create barriers to healthcare. Different models have been developed in the field of health education to determine why an individual is prevented from accepting preventative medical care. The Social Determinants of Health Model says that a person's choices affect their health. Their choices are shaped by the socio-economic structures surrounding them (World Health Organization 2008). Social determinants of health, factors such as the level of poverty in the surrounding population, income, and level of education, are useful predictors of disease rates. However, a person's behavior, and therefore health, is also influenced by other beliefs and attitudes he or she holds. As the physician-sociologist Paul Farmer wrote, to understand the dynamics and distribution of suffering "one must imbed individual biography in the larger matrix of culture, history, and political economy" (Farmer 2005, 41). An ecological model outlook suggests that to adequately explain some behavior it is necessary to study the environment in which the behavior took place and, especially, the information that connects a person to their environment. A person's environment entails the cultural perceptions and expectations that shape an individual's worldview.
The issue of treating HIV/AIDS in the Deep South is compounded by the region's unique problems. Doctors Anderson, Chandra and Mosher (2005) noted the difficulty of treating HIV/AIDS in rural areas in 2005. 42.2% of the Deep South population lives in rural areas, compared to 24.8% nationally. Males living in rural areas, however, are only 41.6% likely to get tested for HIV/AIDS, compared to 49.3% in urban areas (Anderson et al. 2005, 15). Nationally, males in the Deep South are among the least likely to get tested (46.3%) compared to a high of 48.5% in the West (Anderson et al. 2005, 15). Delayed diagnosis and treatment increases the likelihood of the disease spreading, and an under-counting of HIV/AIDS cases further complicates healthcare providers' allocation of resources and their response.
Another factor that must be examined in understanding the disease's spread is the region's high incarceration rate and the possibility of infection of the general population through released prisoners. This was examined by Hammett and Drachman-Jones in 2006. Incarceration rates in the South (790 per 100,000) are the highest in the country (Hammett and Drachman-Jones 2006, 17). Additionally, approximately one fourth of all people in the United States who are living with HIV or AIDS in a given year pass through a correctional facility that same year (Hammett and Drachman-Jones 2006, 17). The South has the highest overall number, though not rate, of HIV infections among correctional releases (Hammett and Drachman-Jones 2006, 19). Patterns of incarceration may mirror the emerging racial pattern of infection. Blacks and Latinos are vastly overrepresented among correctional inmates. Blacks make up approximately 13% of the U.S. population but over 40% of jail and prison inmates (Hammett and Drachman-Jones 2006, 20).
In 2006, Reif, Geonnotti, and Whetten wrote the most comprehensive review of statistics explaining the spread of HIV/AIDS in the Deep South. They expanded on the unique problem posed by the Deep South's rural population by describing several interlocking, multifaceted health indicators that leave the region more vulnerable to disease and poor health. They note that the Deep South states are ranked at the bottom of nearly every national health index, including diabetes, stroke, infant mortality, and sexually transmitted infection (STI) rates. A population already in poor health is particularly vulnerable to the HIV/AIDS epidemic. Five of the ten states with the highest rates of chlamydia and four of the ten states with the highest syphilis rates were in the Deep South (Reif, Geonnotti, Whetten 2006, 971). They note that STIs have been consistently found to facilitate HIV transmission.
Another factor is the endemic poverty of the region. Poverty has been recognized as a barrier to health care that inhibits access to preventive services and treatment. The Deep South states contain the highest rates of poverty in the country. Reif, Geonnotti, and Whetten (2006) extend their argument to explain the health disparities between Whites and Blacks. In the Deep South African-Americans rank far lower, compared to Whites, on measurements of income and poverty rates, and are therefore more vulnerable to poor health. Nationally, half of African-Americans rank 200% below the poverty line (Reif, Geonnotti, Whetten 2006, 972). However, if STDs, poverty, and rural population were the only factors responsible for HIV/AIDS, then similar HIV/AIDS rates should be seen across the Midwest, which is not the case. The authors conclude, "There may be an association of disease with the unique history and culture of the Deep South" (Reif, Geonnotti, Whetten 2006, 972).
The Anderson (2005), Hammett and Drachman-Jones (2006), and Reif, Geonnotti, and Whetten (2006) articles explain the structural barriers that must be overcome to receive care and illustrate social determinants of health that are conducive to the infection's spread. However, a healthcare provider's response based solely on the above articles would only have the intended effect if the healthcare provider could assume that prevention measures and the disease itself were perceived in the same way by everyone. Without taking into account the psychological, cultural, and inherent "submerged" barriers to healthcare access, healthcare providers will be hindering their own efforts. How the disease is perceived by different groups of people living in the Deep South when placed in the context of their life experiences, daily interactions, and religious beliefs must also be taken into account.
In the Deep South the perceptions of HIV/AIDS is different and how information about it is received, differs depending on race. Across all groups, stigma is associated with HIV/AIDS. However, in the African-American community HIV/AIDS is associated with government conspiracy theories and more strongly tied to stigma. Writing in 1991 before the HIV/AIDS rate skyrocketed in the Deep South, Thomas and Quinn (1991) believed that the HIV/AIDS epidemic's effect on the Black community could not be explained without taking into account the mistrust of health officials resulting from the Tuskegee Syphilis Study. They contended that this mistrust fueled government conspiracy theories about HIV/ AIDS, creating another barrier to care.
The Tuskegee Syphilis study was conducted in Tuskegee, Alabama over the course of 40 years, from 1932 to 1972. During the study 399 Black men with syphilis were examined for 40 years and prevented from receiving medication, even after penicillin became available, or being told of their disease. The study was conducted by the Center for Disease Control, the Alabama State Health Department, and the Macon County Board of Health. The authors note that even as late as 1969:
The CDC convened a blue-ribbon panel to discuss the Tuskegee study. The group reviewed all aspects of the experiment and decided against treating the men. This decision ended debate on the Tuskegee study's future: It would continue until 'end point' (Tomas and Quinn 1991, 1501).
When it was exposed in 1972 the study sent shock waves across the country. Thomas and Quinn (1991) contend the study has had a devastating impact on how the African-American community views healthcare providers by fueling conspiracy theories that HIV/AIDS is a weapon of genocide against the Black community. The authors observed that in presentations at public health professional meetings and in interactions with Black community based-organization staff members, "the Tuskegee Study is used to undermine trust and justify AIDS conspiracy theories" (Tomas and Quinn 1991, 1502). Though the fear in the Black community of professional healthcare providers is misplaced, its origin is legitimate. Indeed, "It must be acknowledged that public health research and practice operate in an environment influenced by societal values and political ideology" (Tomas and Quinn 1991, 1504). As HIV/AIDS disproportionately infects the Black population, understanding the context in which Black Americans perceive the disease will be essential so that an effective response can be given.
The Tuskegee Syphilis Study affected not only how African-Americans trusted healthcare providers, but also how African Americans participated in high-risk sexual behavior. In 2006, Ross, Essien, and Torres examined the legacy of the Tuskegee Syphilis among four racial groups using a questionnaire and a random street sample in Houston. Participants were asked if "AIDS is an agent of genocide created by the United States government to kill off minority populations" (Ross, Essien, and Torress 2006, 2). The study found that widespread beliefs in HIV conspiracies occur across different racial and ethnic groups, but was most evident in African-Americans (Ross, Essien, and Torress 2006, 3). Also, genocidal conspiracy beliefs among African American men were associated with a reduction in condom use (Ross, Essien, and Torress 2006, 3).
A similar study, conducted by Williams and Sallar (2010) in Mississippi, also found a correlation between conspiracy theories and condom use. The researchers examined how myths, misconceptions, and prior knowledge of HIV/AIDS impacted sexual behavior among African American men in both a rural and urban setting. The study "revealed that the overall respondents' HIV/AIDS knowledge did not translate into positive attitude or behavior" (Williams and Sallar 2010, 1147). Their knowledge did not translate into the predicted behavior, which led the researchers to conclude that other myths or beliefs were being taken into account. Among participants from the rural Mississippi Delta, who were relatively well informed about HIV/AIDS prevention and causes, more than "40% of the rural men responded negatively to the use of condoms at any time during sexual intercourse" (Williams and Sallar 2010, 1147). Many of the participants did not express any confidence in condoms' ability to prevent HIV.
In addition to conspiracy theories, various studies have demonstrated that stigma in the Deep South is associated with STIs and HIV/AIDS, which is compounded in rural communities. In Sutton, Anthony, Villa, and Weidle's 2010 survey of health care clinics, participant healthcare providers were asked to list perceived barriers to health care. A common response was perceptions of patients' lack of trust in system privacy and confidentiality and their concern about HIV-related stigma (Sutton et al. 2010). Free responses revealed that there is a lot of potential for breaches of confidentiality that may occur when a health department is located in a small town or rural community. Patients were concerned about being identified entering or exiting an HIV testing facility or being recognized by health department staff. Healthcare providers also reported that efforts to heighten HIV awareness, education, and prevention were sometimes hindered by religious and moral objections to HIV education (Sutton et al. 2010).
Lichtenstein, Hook III, and Sharma's 2005 survey of households in the Bible Belt state of Alabama explored how stigma is associated with STIs, which we can expect to be similar to stigma associated with HIV/AIDS and different across gender, race, and church attendance. The survey revealed a gap in perceptions between the African-American community and other ethnic groups. This gap does not bode well for HIV/AIDS prevention among the African-American community. African-Americans and church-goers (regardless of race) who attend church regularly were the two groups most likely to see STIs as a sign of immorality (Lichtensetin, Hook III, and Sharma 2005, 48). African Americans were more frequent churchgoers than Whites (81 % versus 60%) (Lichtensetin, Hook III, and Sharma 2005, 50). Stigma discouraged and impeded two common disease tracking and prevention methods; partner notification and contact tracing. Almost half (45%) of all respondents (African-Americans and Whites) said they would be reluctant to report names for partner identification to the health department, but African-Americans were more likely than Whites to say that they would not seek treatment at all (Lichtensetin, Hook III, and Sharma 2005, 50).
Greater stigma among African-Americans warrants greater investigation, which means the investigation arrives at the doorstep of the Black Church. In the Deep South, the church is the heart of the Black community. When Foster, Cooper, Parton, and Meeks (2011) interviewed Alabama pastors about the role the Black Church could play in spreading HIV/AIDS awareness, many pastors said that they personally were interested in such a project, but they felt that they were prevented from doing so because stigma continued to be an issue for their congregations. One pastor related; "People are afraid to address HIV/AIDS because it may put a dark cloud over your ministry…people will gossip and say, what they talking about that for, they must have a member who is infected" (Foster et al. 2011, 325).
These articles explore possible causes for the vulnerability of the African-American population to the spread of HIV/AIDS. They approach the issue from two very different viewpoints. The first set of articles employ a litany of statistics to list the barriers preventing access to health care for the individual, while the second set of articles places the individual within the context of their community's perceptions and cultural worldview. The structural barriers of poverty and poor health infrastructure prevent people from reaching the health care they need, but the intangible presence of misinformation and stigma channels the disease through a person's networks and relations, fueled by silence and distrust.
Hypothesis
I hypothesize that race will be the most important variable in predicting the spread of HIV/AIDS. The HIV/AIDS virus has devastated minority populations. The U.S. African-American population is concentrated heavily in the Deep South. 54.8 percent of the total U.S. African-American population lives in the Deep South and 18.8 percent lives in the Midwest (The Black Population 2000). The literature suggests the culture and history of the Deep South, including conspiracy theories and stigma in the African-American community, influence the spread of the disease.
Methodology
In order to discern the effects of various social determinants on the spread of HIV/AIDS in poor rural communities, a quantitative correlative analysis of selected statistics of variables at the county level was conducted. The dataset employed contained different socio-economic variables and HIV/AIDS rates for counties from four states, two representing the Midwest and two representing the Deep South. In order to build a dataset that generated statistically relevant results, a sufficient number of counties were necessary. The dataset combined counties from all four states instead of analyzing them as two separate datasets because it was the only method in which a sufficient number of counties were achieved.
There is a problem with only using counties from the Deep South because rural counties in the Deep South are heavily segregated along racial and economic lines; White counties are far richer compared to Black counties. In the Mississippi Delta and in the Alabama Black Belt, counties are nearly 70 % to 80% African-American and among the poorest in the country. Counties from the Midwest were chosen because it was the only other region in the United States where equally poor, rural counties were found that were not uniformly African-American, thus facilitating the statistical analysis.
The quantitative method used is based in part on a paper by Song, Hall, Harrison, Sharpe, Lin, and Dean (2011). Their study developed a system demonstrating how correlation and partial correlation coefficients can be used to measure the impact of socioeconomic factors on AIDS diagnosis rates in certain geographic areas nation-wide. Out of 12 variables, they found the AIDS diagnosis rate was highly correlated with the distribution of race, population density, and marital status in an area (Song et. al. 2011). The study concluded that area-based measures of socioeconomic variables can be used to identify risk factors associated with AIDS. In the course of their study they noted that while correlation analysis is used to identify risk factors, confounding from other variables must be taken into account.
Data Sources
The American Community Survey. While the U.S. Census provides demographic information once every ten years, the U.S. Census American Community Survey provides data every year depicting a variety of subjects. The information is down to the census tract level and captures demographic and socio-economic information including variables such as age, education, employment, housing, income, mobility, country of origin, language spoken at home, and poverty (American Fact Finder). Information provided was from the 2005-2009 American Community Survey 5-Year Estimates dataset. The 2005-2009 dataset is more accurate for small population levels.
Geographic area. Four states, Alabama, Mississippi, Oklahoma, and Ohio, were chosen for analysis, two representing the Deep South and two representing the Midwest. Mississippi was chosen because of its particularly high HIV/AIDS rate, and Oklahoma was chosen because its per capita income is comparable to Alabama and Mississippi's (United States and States, Median Household Income 2007). The other states were chosen based on the ease of finding publicly available HIV/AIDS data released by their respective state health departments.
The county level was chosen to best capture the impact of the socio-economic variables because demographic make-up can vary widely from one part of a state to another. Additionally, cities can distort data and this research focused only on rural populations. Counties with more than 50,000 people were designated urban and excluded from the data set. This loose definition was derived from the definition utilized by the 2010 U.S. Census (2010 Census Urban and Rural Classification and Urban Area Criteria).
HIV/Aids Surveillance Data. The spread of HIV/AIDS was measured by incidence rate. Incidence rate is defined as the number of new HIV infections in a specific population in a given year. This is uniformly measured at a rate per 100,000. State Health Departments receive funding from the Centers for Disease Control and Prevention (CDC) to compile and report all incidents of HIV/AIDS infection (HIV Surveillance Report). The data for each individual county was compiled by visiting each state's representative state health department website. HIV/AIDS incidences from 2008 and 2009 were used for Alabama and Mississippi, and from 2009 for Oklahoma and Ohio, with the discontinuity a result of trouble finding publicly available data (Public Health Areas January-December 2008, Mississippi HIV Rates 2006-2010, Harris 2009, 2009 HIV Public Surveillance Data For Ohio). County-level rates per 100,000 were not provided by the Ohio Health Department. These rates were calculated using the 2005-2009 American Community Survey Population data. In sparsely populated areas there may be too few data points causing HIV/AIDS incidence rates to vary widely from one year to the next. To prevent against this for Mississippi and Alabama counties, an average of the 2008 and 2009 HIV/ AIDS incidence rates per 100,000 was compiled. Due to a lack of available data this operation was not repeated for Oklahoma and Ohio.
Data Analysis
First, data from the 2005-2009 American Community Survey 5-Year Estimate was used to measure relevant social determinant health variables. Except for per capita income, all of the variables were compiled as percentages. For example, the percent of the population 25 years and older with some college education was calculated by dividing the number of people 25 years and older with some college education by the number of people 25 years and older in the county.
The following demographic, social, and economic variables were selected:
- HIV/AIDS rate per 100,000 (HIV/AIDS Rate)
- Percent of county that is Black (Percent of County that is Black)
- Percent of county with some college education, 25 years and older (College Education)
- Per capita income (Per Capita Income)
- Percent of the population that lives below the poverty rate (Poverty Rate)
Additionally, the following variables were collected for descriptive purposes:
- Total population
- Black per capita income as a percent of White per capita income
- HIV/AIDS cases in 2008
This data was combined at the county level.
After the data set was constructed, and the urban counties had been removed, a matrix scatter plot was created to visually depict the relationship between the four Social Determinant Health variables and the HIV/AIDS rate. A scatter plot can reveal whether there is a linear correlation between variables. A strong negative correlation was predicted between the demographic variable Percent of County that is Black and the Social Determinant Health variables of per capita income, and percent of the population living below the poverty line. A bivariate correlation was conducted to determine the strength of the relationship between the variables, and whether the relationship is statistically significant.
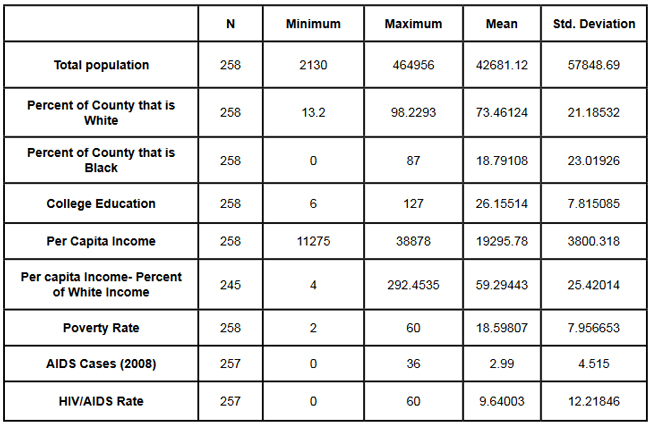
A major problem of measuring the correlations between variables is that often demographic variables are strongly correlated with other social determinant health variables. In this research project it is particularly hard to discern the effects of different variables in the Deep South, because African-Americans are disproportionately at the bottom of the socio-economic ladder. As noted earlier in this paper, nationally, half of African-Americans rank 200% below the poverty line (Reif, Geonnotti, Whetten 2006, 972). This statistic demonstrates the reality described by one writer when he says "America is a place where class historically coincides with race. [This] is the heaviest legacy of slavery and segregation" (Bolina 2011). In Mississippi and Alabama, Black per capita income is on average half the per capita income of Whites (Table 1). Accordingly, what appears to be a correlation between two variables could actually be one variable appearing to correlate with the dependent variable because of its close relationship with a third variable. To adjust for this, a partial correlation was conducted. A partial correlation calculates coefficients that describe the linear relationship (correlation) between two variables while accounting for the effects of one or more additional variables.
After measuring the degree of correlation and after taking into account the indirect effects of other variables, a multiple linear regression was performed. A multiple linear regression specifies the nature of the relation between the variables and measures to what extent the independent variables are predictive of the dependent variables.
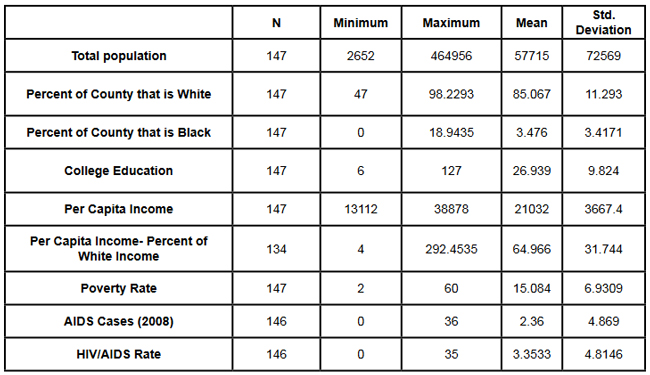
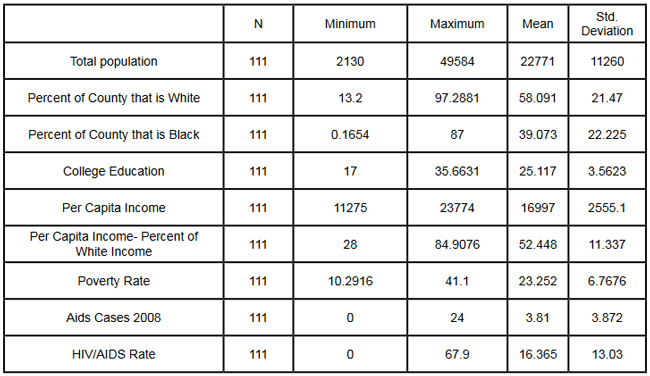
Results
With all four states combined the dataset included 258 counties (Table 1). Of these 258, 111 were from the Deep South, and 147 were from the Midwest (Tables 2, 3). The regional differences in the datasets mirror publicly reported data. Mean per capita income was almost $10,000 higher in the Midwest. In the Deep South HIV/AIDS Rates, as measured per 100,000, were higher at 16.36 compared to 3.35 in the Midwest. Also, in the states examined, African-Americans made up an average of 39 percent of the population in Deep South counties compared to an average of 4 percent in Midwest counties. In both regions, African-Americans are significantly poorer on average than Whites, and the education rate is nearly identical. It must be noted that this is an extremely poor population with per capita income never rising more than $39,000, and ranging as low as $11,275. On average, nearly 22 percent of the population captured in this dataset lived at or below the federal poverty level, with one county as high as 60 percent.
{kind=link}
{kind=link}
{kind=link}
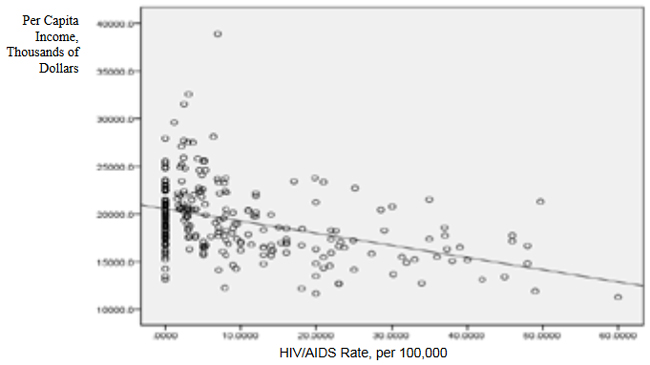
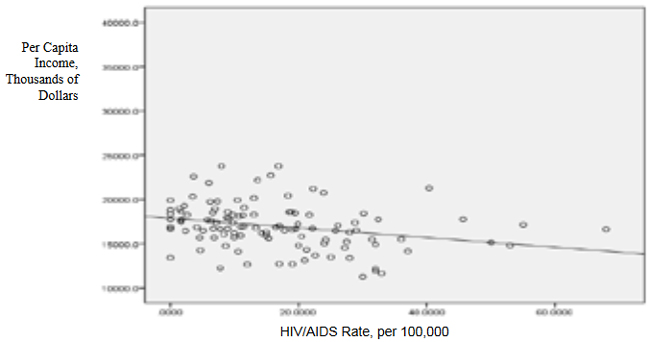
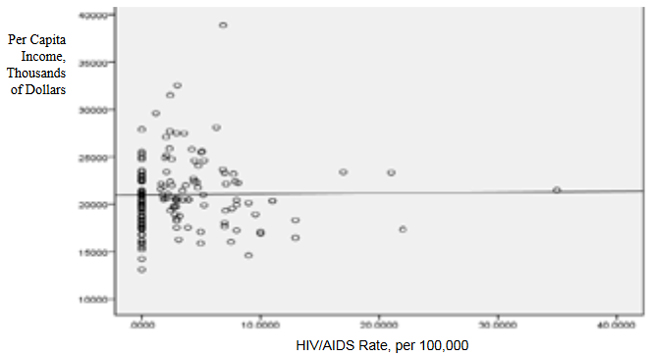
From examining the regional data and noting the differences in poverty and HIV/AIDS between them, it at first seems there must be a correlation between income and HIV/AIDS. Per capita income especially is often considered to be an indicator of a population's susceptibility to disease. This relationship was examined more closely in a scatter point graph of all four states (Graph 1), which appears to indicate there is a negative correlation between per capita income and HIV/AIDS rates. This correlation also appears when the Southern states are examined (Graph 2). There does not appear to be a negative correlation for the Midwestern States (Graph 3). It should be noted, however, that for all four states the per capita income is very low but there is not a large range of income. The small range in income may not provide an adequate variety of data points.
{kind=link}
{kind=link}
{kind=link}
All four independent variables were associated with the dependent variable in a scatter point matrix (Graph 4). Education appears to be irrelevant but otherwise there appears to be a linear correlation between the other independent variables and HIV/AIDS per 100,000. Additionally there appears to be linear correlations between all of the social determinants of health variables and the percent the percent of the county that is Black.
{kind=link}
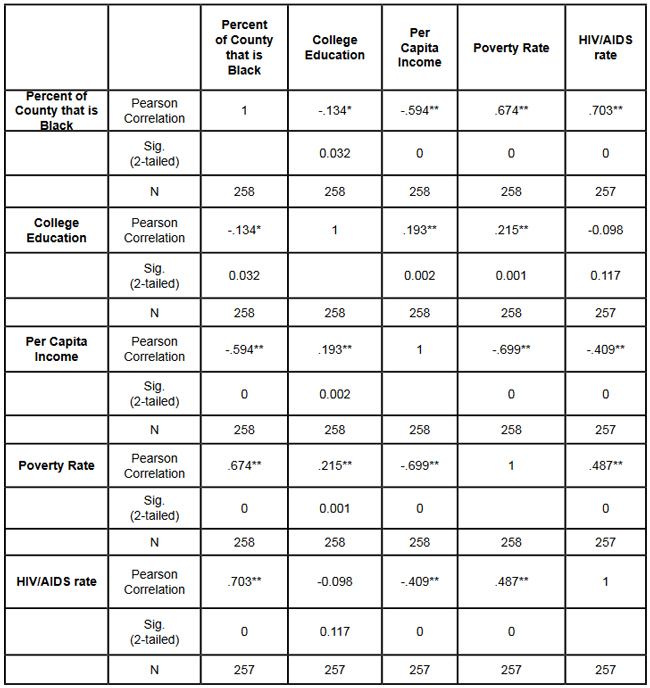
The correlations between the independent variables and HIV/AIDS rate per 100,000 were then measured using a bivariate correlation procedure (Table 4). A bivariate correlation determines the strength of the relationship between the variables, and whether the relationship is statistically significant. All variables with a significance of <.05 were considered statistically significant, with .000 considered especially significant. The significance of the correlations between the variables and HIV/AIDS Rate was .000 for all variables except for the percent the of population 25 years and older with some college, which, at a significance of .117 was not significant. Of the correlations that were statistically significant the strength of their correlation with HIV/AIDS Rate ranged from per capita income at -.409 to .703 for the percent of the county that is Black. It is interesting to note that not only did the percent of the county that is Black have the strongest correlation with HIV/AIDS, but it also had strong correlations with the other variables.
{kind=link}
Table 4: Bivariate Correlations. *Correlation is significant at the 0.05 level (2-tailed). **Correlation is significant at the 0.01 level (2-tailed).
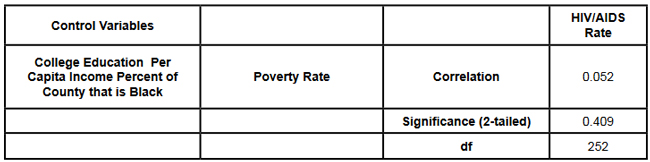
The partial correlation procedure was performed to examine variables' correlations with the HIV/AIDS Rate variable while controlling for other variables. There was no significant change in the strong correlation between the percent of the county that is Black and HIV/AIDS, which remained at around .62 (Table 5)
{kind=link}
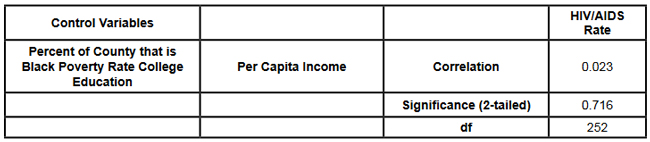
However, the other three variables were all found to be statistically insignificant in regards to having a correlation with the HIV/AIDS Rate (Tables 6, 7, 8). A significance of .05 or less must be attained for correlation to be considered statistically significant, but for the economic variables and for education the significance ranged from .432 to .716.
{kind=link}
{kind=link}
{kind=link}
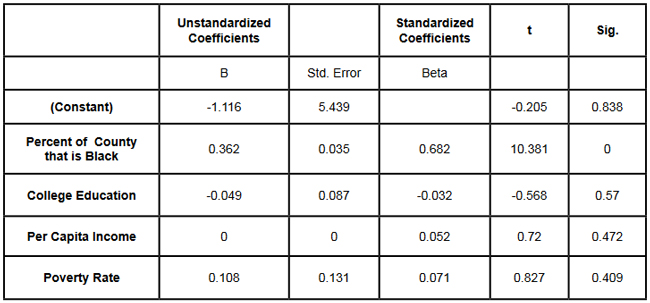
Lastly, a linear regression was produced to check for continuity in results and to measure the specific relationship between the variables and the dependent variables (Table 9). The results from the linear regression agreed with the results from the partial correlations that education and the economic variables were not statistically significant. From the adjusted R square value in the model summary we know that the independent variables explain almost 50% of the data points. While not extremely high, it is significant enough to signify that the variables are relevant. In the coefficients table displaying the independent variables, the only significant one (.05 or less) is the percent of the county that is Black. The coefficients table also informs the reader that for every 1 unit increase in Black population, there is a predicted .682 unit increase in HIV/AIDS Rate per 100,000.
{kind=link}
{kind=link}
There is a very complicated relationship between race and poverty, income, and education. These variables influence each other in different ways. However, after controlling for race, there was found to be no statistically significant correlation between education, income, or poverty and HIV/AIDS in the sample counties. Instead of various social determinant health variables, the strongest correlation with HIV/AIDS Rate was found between the demographic variable, the percent of the county that is Black.
Implications
This research shows that within poor, rural counties, race is the variable that explains the rapidity of the disease's spread or the magnitude of its destruction. Inherited cultural and historical factors in the African-American community must be examined. I propose that additional qualitative research is necessary to explore whether lingering conspiracy theories surrounding the Tuskegee syphilis experiments, coupled with social stigma, carry explanatory power in understanding the persistent phenomenon of elevated HIV/AIDS rates. The following proposal for qualitative research is grounded in an interpretative paradigm that there are multiple realties of the world according to different perceptions. In conducting his field research the researcher would focus on social relationships and the meaning and symbolism attached by people to interactions in their daily lives.
Invisible barriers often exist for marginalized groups such as minorities or poor people in a variety of venues, from the doctor's examination room to public health campaigns. In the examination room, White and middle-class patients may experience the interaction differently because they "seem able to create workable relationships with healthcare providers because of their ability to pay for services or utilize private insurance and because they have cultural support" (Heller et al. 2004, 32).
My proposed research agenda approaches a public health issue from a development perspective. Vulnerable populations are often the most marginalized groups in a society. Implementing development programs to effectively reach vulnerable populations (or a failure to so) depends on the ability of a program to bridge ethnic, religious, gender and class lines and to facilitate cross-cultural communication. This proposed research would build on previous work like Williams and Sallar's 2010 studies in Mississippi, which revealed discrepancies between how African-American men understood HIV/AIDS and their resulting behavior, and Lichtenstein, Hook III, and Sharma's surveys in Alabama, which revealed differences in how HIV/AIDS is perceived among different racial groups.
I propose conducting a series of semi-structured interviews and focus groups and applying discourse analysis to test whether conspiracy theories from the Tuskegee Syphilis Study and stigma can further explain the spread of HIV/AIDS. By employing interviews a researcher would better understand different perceptions. Through discourse analysis applied to focus groups, a researcher may be able to understand how behavior is affected and deduce additional factors in the disease's spread that have not been considered previously.
Health departments in the Deep South are failing their citizens in enacting measures to control a disease's spread. In the face of the fastest growing HIV/AIDS rates in the country Alabama, Georgia, and Mississippi spend $10,413, $16,647, and $13,609 per patient respectively compared to a national average of $24,867 (Medicaid and HIV: A National Analysis 2011 ). More troubling is the example of the state of Mississippi's refusal to accept federal funds to fight HIV/AIDS, including Governor Haley Barbour's "attempt to block health care reform that would expand Medicaid benefits for people living with HIV in the state" (Rights at Risk 2011, 2). A report by the Human Rights Watch found that the state of Mississippi "leave[s] people with HIV/AIDS without treatment at rates comparable to those in Botswana, Ethiopia, and Rwanda" (Rights at Risk 2011, 2).
A qualitative, ethnological research agenda identifying areas of miscommunication could provide a unique insight into this pressing public health crisis by helping doctors understand the fears of their patients, helping communities develop a prevention plan, and helping policy makers allocate resources more efficiently. There is an urgent need for more research that can contribute to better understanding how the HIV/AIDS virus spreads through these communities. Beneath the numbers and graphs it is more important to remember that these values represent glimpses into lives. They capture the extremes, the mean of a middle class existence, the depths of poverty, and the blending of race, blood, and disease.
References
2009 HIV Public Surveillance Data. State of Ohio HIV Infections Annual Surveillance Statistics. Ohio Department of Health.
2010 Census Urban and Rural Classification and Urban Area Criteria. The U.S. Census Bureau. http://www.census.gov/geo/www/ua/2010urbanruralclass.html
American Fact Finder. Subject Tables. U.S. Census Bureau. http://factfinder.census.gov/servlet/STSelectServlet?_ts=341355082029
Anderson, John E., Anjani Chandra, and William D. Mosher. 2005. HIV Testing in the United States, 2002. Advance Data from Vital Health and Statistics. The Center for Disease Control. Nov. 8. No. 363.
The Black Population 2000. U.S. Census Brief. 2001. August. http://www.census.gov/prod/2001pubs/c2kbr01-5.pdf. Access on 3/18/2012.
Bolina, Jaswinder. Writing like a White Guy, On Race, Language and Poetry. Poetry Foundation. http://www.poetryfoundation.org. Accessed on 3/18/2012.
Farmer, Paul. 2005. Pathologies of Power, Health, Human Rights, and the New War on the Poor. Berkley and Los Angeles. University of California Press.
Foster, Pamela, Krista Cooper, Jason M. Parton; and John O. Meeks. 2011. Assessment of HIV/AIDS Prevention of Rural African American Baptist Leaders: Implications for Effective Partnerships for Capacity Building in American Communities. Journal of the National Medical Association. April. Vol. 103, No. 4. 323-331.
Hammett, Theodore, and Abigail Drachman-Jones. HIV/AIDS, Sexually Transmitted Diseases, and Incarceration Among Women: National and Southern Perspectives. Sexually Transmitted Diseases. Vol. 33, Issue 7. Jul, 2006.
Harris, Terrainia, etc. 2009 Oklahoma HIV/STD Comprehensive Epidemiologic Profile. Oklahoma State Department of Public Health. Oklahoma City, Oklahoma.
Heller, Daliah, Kate McCoy, and Chiazo Cunnigham. 2004. An Invisible Barrier to Integrating HIV Primary Care with Harm Reduction Services: Philosophical Clashes between the Harm Reduction and Medical Models. Public Health Reports. January – February. Vol. 119. 32-39.
Lichtenstein, Brownen, Edward W. Hook III, and Amit K. Sharma. 2005. Public Tolerance, Private Pain: Stigma and Sexually Transmitted Infections in the American Deep South. Culture, Health, and Sexuality. Vol. 7, Issue 1. 43-57.
McKinnon, Jesse. The Black Population, 2000. Census Brief. U.S. Department of Commerce. Economics and Statistics Administration. U.S. Census Bureau. August 2001.
Medicaid and HIV: A National Analysis. The Kaiser Foundation. 2011. October. http://www.kff.org/hivaids/upload/8218.pdf.
Mississippi HIV Rates 2006-2010. Mississippi HIV Statistics. Mississippi State Department of Health. http://msdh.ms.gov/msdhsite/_static/31,0,150,134.html
Public Health Areas (January-December 2008). Alabama AIDS and HIV Quarterly Statistics. Alabama Department of Public Health. http://www.adph.org/aids/
Reif, Susan, Kristen Geonnotti, and Kathryn Whetten. HIV AIDS and Infection in the Deep South. American Journal of Public Health. June 2006, Vol 96, No. 6. p. 970.
Ross, Michael, James Essien, and Isabel Torres. 2006. Conspiracy Beliefs about the Origin of HIV/AIDS in Four Racial/Ethnic Groups. Journal of Acquired Immune Deficiency Syndrome. March. Vol. 41 No. 3. 342-344.
Song R, Hall H, Harrison K, Sharpe T, Lin L, and Dean H. 2011. Identifying the Impact of Social Determinants of Health on Disease Rates Using Correlation Analysis of Area-Based Summary Information." Public Health Reports. Volume 126. Supplement 3.
Sutton, Madeline, Monique-Nicole Anthony, Christie Villa, and Paul Weidle. 2010. HIV Testingand HIV/AIDS Treatment Services in Rural Counties in 10 Southern States: Service Provider Perspectives. The Journal of Rural Health. Vol. 26. 240-247.
Thomas, Stephen B and Sandra Quinn. 1991. The Tuskegee Syphilis Study, 1932 to 1972: Implications for HIV Education and AIDS Risk Education Programs in the Black Community. American Journal of Public Health. November. Vol 81, No. 11.
United States and States, Median Household Income. The 2007 American Community Household Survey 1-year estimates. U.S. Census Bureau. http://factfinder.census.gov/servlet/GRTTable?_bm=y&-_box_head_nbr=R1901&-ds_name=ACS_2007_1YR_G00_&-_lang=en&-format=US-30&-CONTEXT=grt
Williams, Patrick, and Anthony M. Sallar. 2010. HIV/AIDS and African American Men: Urban-Rural Differentials in Sexual Behavior, HIV Knowledge, and Attitude towards Condoms Use. Journal of the National Medical Association. Dec. Vol. 102, No. 12.
World Health Organization, Commission on Social Determinants of Health. 2008. Closing the Gap in a Generation: Health Equity Through Action On The Social Determinants of Health. Geneva: WHO. Also available from: URL: http://www.who.int/social_determinants/thecommission/finalreport/en/. [cited 2011 Dec 7].